
Incorporating the Social Determinants of Health in Practice to Address Sexual and Reproductive Health for Young People Involved in Foster Care


Overview
This brief aims to provide child welfare practice professionals (e.g., caseworkers) information about the social determinants that influence young peoples’ sexual and reproductive health and offer them guidance on incorporating this knowledge in daily practice.
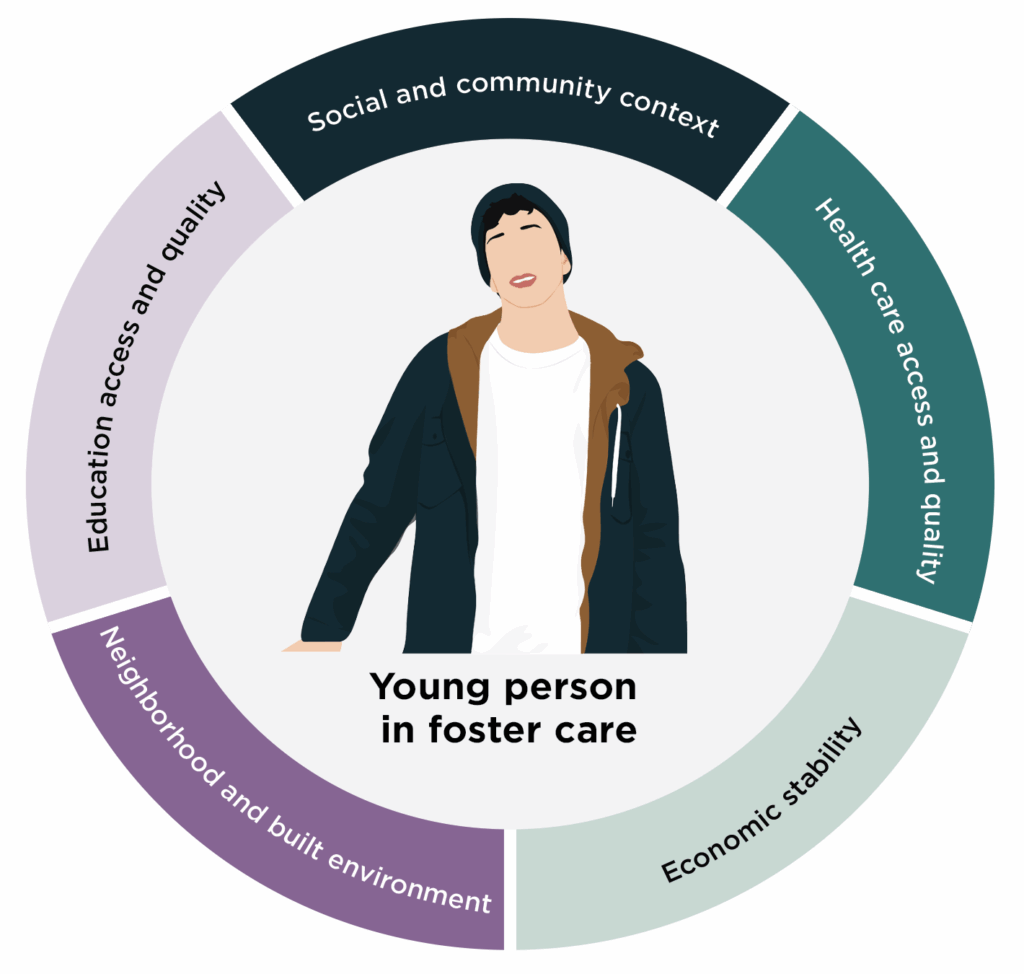
Social determinants of health are the social, economic, and environmental conditions present in communities where people live, work, and gather.[1],[2] Social determinants of health cover five key areas:
- Neighborhood and built environment
- Education access and quality
- Health care access and quality
- Economic stability
- Social and community contexts
While these conditions can affect young people’s sexual and reproductive health experiences and access to services in all communities,[3] their effects may be amplified for young people in foster care.[4] See the full brief for a discussion of how the social determinants of health influence teen pregnancy and related sexual and reproductive health experiences of young people in foster care. Addressing the social determinants of health is important for providing youth in foster care with effective services to improve youth outcomes.
See these practice tips for navigating the social determinants of health when working with youth in foster care.
Suggested Citation: Rosenberg, R., Woods, N., Naylon, K., & Tallant, J. (2022). Incorporating the social determinants of health in practice to address sexual and reproductive health for young people involved in foster care. Child Trends. https://activatecenter.org/resource/incorporating-social-determinants-of-health-and-in-practice-to-address-sexual-and-reproductive-health-for-young-people-involved-in-foster-care/
This page was last updated in January 2026.
Related Resources